ALIF Surgery: Anterior Lumbar Interbody Fusion
There are various surgical methods that can help alleviate back pain by fusing two or more spinal vertebrae together. One technique is known as ALIF surgery or anterior lumbar interbody fusion.

What is ALIF surgery?
Anterior lumbar interbody fusion (ALIF) is a spinal fusion procedure in which surgeons navigate through the abdomen to access the front of the spine and fuse two or more vertebrae in the lower back together. The procedure involves an “approach” surgeon (who provides access to the spine) and a spine surgeon, working together.
The lumbar portion of the spine contains the five spinal vertebrae (L1 to L5) of the lower back. An ALIF procedure may also involve the intervertebral disc located between the L5 vertebra and the highest vertebra (S1) of the sacral spine that includes the sacrum and coccyx (tailbone). This is known as an L5/S1 ALIF.
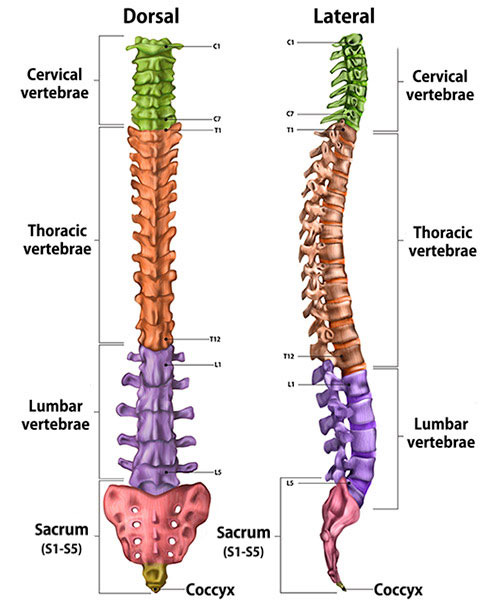
Illustration of cross-section of spine, dorsal (back to front) and lateral (side) views, showing its vertebral sections.
What conditions does ALIF surgery treat?
The best way to think about ALIF surgery is that it is used to restore the vertical space between two spinal vertebrae. When a lumbar disc degenerates, the space between the two vertebrae it nests between is compromised. This can lead to a pinched nerve, instability, arthritis or spinal deformity. Thus, ALIF can be used to treat radiculopathy (a pinched nerve), degenerative disc disease, spondylosis (spinal arthritis), spondylolisthesis (instability), and spinal deformities such as degenerative scoliosis.
Who is a good candidate for ALIF surgery?
The best candidates for ALIF surgery are people experiencing disc collapse at the lowest lumbar segments of the spine (L4/5 and L5/S1) who need the maximum restoration of height in that disc space to relieve the cause of their pain.
While it is possible to perform ALIF at upper lumbar levels (L1/2, L2/3, L3/4), it is more challenging and comes with a higher risk of complications. When a restoration of disc space is needed at upper lumbar levels (L1/2, L2/3, L3/4), lateral lumbar interbody fusion (LLIF) or transforaminal lumbar interbody fusion (TLIF) are usually better options.
Ultimately, the decision to use ALIF or another interbody fusion technique (TLIF or LLIF) is highly dependent on the patient’s individual anatomy and the type of pathology to be addressed.
Finally, given that the procedure requires a general or vascular surgeon to access the spine through the abdomen, very obese patients or those with a history of extensive prior abdominal surgeries are poor candidates. (Find a surgeon at HSS who performs lumbar spinal fusions to learn whether this surgery may be appropriate for you.)
How is ALIF surgery performed?
There are two major parts to ALIF surgery. Spelling out the acronym – "anterior lumbar interbody fusion" – provides language to describe how the procedure is performed. Part 1 of the surgery (the approach), is performed by a surgeon with expertise in abdominal or vascular surgery to create an anterior (frontal) opening to access the lumbar spine. Part 2, performed by the spine surgeon, involves removing the spinal disc and replacing it with a spacer between the vertebrae (vertebral bodies) to fuse them (in other words, interbody fusion).
Approach
The approach begins with a horizontal or vertical incision on the abdomen. Next, the approach surgeon splits the abdominal muscles and moves the abdominal contents (contained in a covering called the “peritoneum”) to the side. This allows them to visualize the front of the spine, during which they assess the relationship between the spine and major blood vessels (the vena cava, aorta, and common iliac arteries and veins). These vessels supply blood to the legs. Once these vessels are protected with a retractor, the spine surgeon comes in to perform the second part of the surgery.
Discectomy and interbody fusion
The second part of the ALIF is performed by the spine surgeon. In this part of the procedure, the disc is removed from the spine (discectomy), working in an anterior-to-posterior (front-to-back) direction. Sometimes, if there is a substantial bony deformity or spondylolisthesis, part of the front portion of vertebrae will have to be removed as well. A “cage” (that is a, a spacer) is then placed into the empty space where the disc was. This cage is often filled with bone grafting materials. Screws are sometimes placed through the cage to secure it in place.
If the surgeon feels that extra fixation is needed to further stabilize the vertebrae, the incision in the front will be closed and the patient will then be flipped over in order to place posterior screws and rods into the vertebrae (meaning that this instrumentation is inserted from the back toward the front of the spine).
Animation: ALIF spinal fusion surgery
This video provides an illustrated look at the ALIF procedure, which makes space between the vertebral bodies to relieve pressure and create more room for nerves to exit the spinal column.
How long does ALIF surgery take?
The length of an ALIF surgery is extremely variable as it is highly dependent on each patient’s individual anatomy. For people having an L5/S1 ALIF with anatomy that allows for easy access to the front of the spine, the procedure can take one to two hours from start to finish. For patients with prior surgeries, spinal deformities, or anatomy that makes it difficult to access the spine, the surgery can take much longer.
If the patient requires a “flip” in order to place posterior screws and rods, this also adds to the amount of time required for the surgery.
What is the recovery time for ALIF surgery?
At HSS, we like ALIF patients to get up and begin physical therapy on the day of their procedure. For a one- to two-level ALIF with or without posterior fixation, patients will often go home one to three days after surgery. The specifics of activity and recovery should be discussed with their surgeon. Patients are generally prevented from engaging in high-impact activities – such as running, weightlifting, sports (including golf) – until the fusion between the vertebrae is more mature (around three to six months).
Importantly, if an ALIF is performed as part of a larger procedure (such as a deformity correction or multilevel anterior/posterior fusion), the hospital stay can be much longer. This also adds substantial variability to the recovery time.
Do you need physical therapy after an ALIF surgery?
The need for physical therapy is highly dependent on surgeon preference, the patient’s preoperative fitness, and individual recovery course. Some patients may not need physical therapy at all, while others may need many sessions.
How soon can you walk after an ALIF surgery?
At HSS we try to get our patients walking on the day of an ALIF surgery.
How painful is ALIF surgery?
Given that ALIF does not involve disruption of the posterior muscles that cover the spine, the surgery is usually better tolerated than a posterior lumbar fusion.
Is ALIF minimally invasive?
ALIF is considered a minimally invasive surgery as it uses anatomical corridors (surgical access routes) without major disruption of tissue planes, meaning the spaces between, muscles, nerves, organs or other soft tissues.
How big will my ALIF scar be?
ALIF scars are very similar to scars from C-sections. The incision length for an ALIF is dependent on the number of vertebral levels that need to be addressed and the patient’s frame and body type.
In terms of healing, everyone’s skin heals differently. For example, if your body generally forms thick scars, you are more likely than some others to form a thick scar after any surgery. Keeping your surgical incision out of the sunlight for the first year after surgery and using silicone strips can help improve scarring.
What risks or complications can occur with ALIF surgery?
There is generally a low rate of complication after ALIF surgery. Reviews of the spine literature show that the most common complications are ileus (2%), wound infection (1%), retrograde ejaculation (permanent in approximately 1%), and neurologic problems leading to leg pain, numbness, or weakness (1% or 2%). More rare complications include injury to the ureters or bowel.
However, the most serious risk of ALIF surgery is injury to the major blood vessels in front of the spine. Blood vessels are injured in approximately 1% to 2% of cases. Most of the time, these injuries are minor and the approach surgeon repairs the vessel at the time of surgery. In the worst-case scenario, serious or unrepairable injuries to the major blood vessels can lead to loss of limb or even death.
Regarding longer-term complications, failure to heal (pseudarthrosis), hardware failure, or settling of the cage into the vertebral body (a condition known as “subsidence”) can occur and sometimes necessitate a second surgery.
How successful is ALIF surgery?
The majority of studies show that ALIF leads to a successful fusion between the vertebrae in at least 90% of cases, with many studies showing rates of fusion in greater than 95% of cases.
With regard to the success of the surgery in relieving preoperative symptoms, this is highly dependent on the reasons for having the surgery. Patients should speak with their surgeon about their particular case.
Posted: 11/29/2022
Authors

Assistant Attending Orthopedic Surgeon, Hospital for Special Surgery
Instructor in Orthopedic Surgery, Weill Cornell Medical College
Related articles
References
- Body AM, Plummer ZJ, Krueger BM, Virojanapa J, Nasser R, Cheng JS, Prestigiacomo CJ. Retrograde ejaculation following anterior lumbar surgery: a systematic review and pooled analysis. J Neurosurg Spine. 2021 Jul 16;35(4):427-436. doi: 10.3171/2020.12.SPINE201101. PMID: 34271542.
- Phan K, Xu J, Scherman DB, Rao PJ, Mobbs RJ. Anterior Lumbar Interbody Fusion With and Without an "Access Surgeon": A Systematic Review and Meta-analysis. Spine (Phila Pa 1976). 2017 May 15;42(10):E592-E601. doi: 10.1097/BRS.0000000000001905. PMID: 27669042