Total Ankle Arthroplasty in Flatfoot Deformity with Deltoid Insufficiency
From Grand Rounds from HSS: Management of Complex Cases | Volume 8, Issue 2
Case Report
In January 2017, a 69-year-old man with a history of severe flatfoot deformity presented with persistent, localized pain at the anterior aspect of the right ankle, causing progressive disability and difficulty with ambulation. Two years prior, he underwent subtalar and talonavicular arthrodesis, as well as first tarsometatarsal arthrodesis and a gastrocnemius recession to address his flatfoot deformity.
On physical examination, the patient stood with slight valgus alignment in his right hindfoot and ambulated with an antalgic gait. His first ray was stable. He had tenderness at the ankle and talonavicular joints, with a range of 5° of dorsiflexion and 20° of plantarflexion at the ankle. There was no appreciable motion at the hindfoot. Weight-bearing radiographs revealed end-stage arthritis in the ankle joint, with radiolucency and failed hardware at the talonavicular joint (Fig. 1). Single-photonemission computed tomography (SPECT) demonstrated increased activity at the ankle, as well as at the talonavicular joint, thus confirming the presence of talonavicular joint nonunion (Fig. 2).

Figure 1: Weight-bearing lateral radiograph at initial presentation indicating end-stage arthritis in the ankle joint, with radiolucency and failed hardware at the talonavicular joint.

Figure 2: SPECT images showing increased uptake at the talonavicular and tibiotalar joints, confirming the presence of talonavicular joint nonunion.
In May 2017, the patient underwent total ankle replacement and revision talonavicular arthrodesis. A percutaneous Achilles tendon lengthening was performed in order to restore dorsiflexion at the tibiotalar joint.
A fixed bearing, modular stem ankle replacement implant was used to achieve sufficient fixation within the tibia and talus, given the patient’s history of hindfoot arthrodesis. A revision talonavicular arthrodesis was performed through the anterior ankle approach; autograft from the tibial cut, as well as recombinant human platelet-derived growth factor BB (rhPDGFBB), augmented healing (Fig. 3).
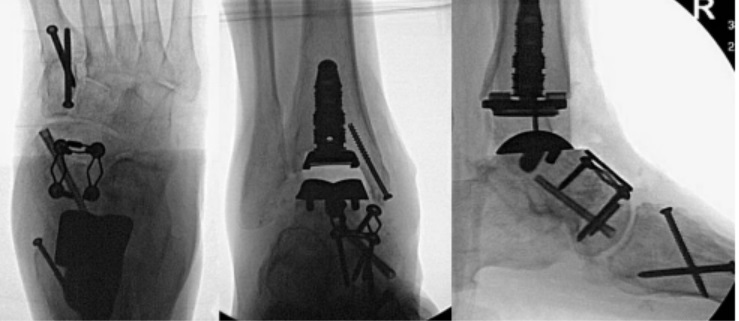
Figure 3: Intraoperative images from May 2017, showing a fixed-bearing, modular stem ankle replacement implant and a revised talonavicular arthrodesis.
The patient’s initial postoperative course was without complication. At the 12-week postoperative visit, weight-bearing radiographs of the ankle demonstrated valgus tilt at the tibiotalar prosthesis (Fig. 4).The patient denied pain at that time and was ambulating fully in a sneaker. A hindfoot alignment view radiograph also indicated slight valgus at the hindfoot (Fig. 5).

Figure 4: Postoperative weightbearing radiograph of the ankle demonstrating valgus tilt of the tibiotalar prosthesis and hindfoot.

Figure 5: Postoperative radiograph demonstrating valgus alignment of the hindfoot.
Weightbearing CT confirmed the valgus deformity at the tibiotalar joint and demonstrated osseous union of the talonavicular joint with intact hardware. Given the severity of the valgus tilt at the tibiotalar prosthesis and concern for the longevity of the prosthesis, reoperation was indicated to reconstruct the deltoid ligament, and a medializing calcaneal osteotomy was indicated to improve hindfoot alignment.
Four months after the total ankle arthroplasty, the patient underwent surgery to restore alignment to the ankle and hindfoot. The polyethylene was removed from the tibiotalar prosthesis. A deltoid ligament reconstruction was performed using a semitendinosus allograft that was docked distally at the sustentaculum tali, tensioned through the tibia and secured with a biotenodesis screw. The polyethylene insert was upsized by 2 mm.
A medializing calcaneal osteotomy was then performed through an oblique incision along the lateral aspect of the calcaneus, and the heel was translated medially to achieve a neutral hindfoot alignment.
One year after the procedures to restore ankle and hindfoot alignment, the patient was doing well, with a well-aligned, balanced ankle prosthesis and a neutral hindfoot (Fig. 6). He ambulated without pain and reported great satisfaction with his overall outcomes.

Figure 6: Final postoperative radiographs of the ankle and hindfoot showing (A) a well-aligned, balanced ankle prosthesis and (B) the hindfoot in neutral position.
Discussion
This case of severe flatfoot deformity in conjunction with progressive ankle arthritis was managed with three surgical procedures. It highlights the importance of ligamentous stability with proper alignment of the hindfoot in ensuring a successful outcome of ankle arthroplasty in a patient with flatfoot deformity and deltoid ligament insufficiency.
In treating ankle arthritis accompanied by significant foot deformity, there is controversy over whether a staged approach is necessary and whether the ankle arthritis or the foot deformity should be addressed first. Although in this case ankle arthritis was noted at the time of the original flatfoot reconstruction surgery, the surgeon performed hindfoot arthrodesis because the majority of pain and deformity was in the hindfoot. Dodd and Daniels describe the necessity of staging procedures in patients who have both flatfoot deformity and end-stage ankle arthritis [3]. They note that one major bony procedure with a total ankle replacement is generally safe, although multiple bony procedures increase the risk of complications. Chan et al. found that the medializing calcaneal osteotomy is the primary determinant of hindfoot valgus correction in flatfoot reconstruction [1]. In addition, Conti et al. showed that achieving 0 to 5 mm varus heel alignment correlated with the best clinical outcomes scores in patients with flatfoot deformity [2].
This case exemplifies a complex deformity requiring management of both bony deformities and ligamentous incompetence. After ankle replacement and revision talonavicular arthrodesis, the talar component tilted into valgus, revealing deltoid ligament insufficiency not appreciated at the time of the ankle arthroplasty. Deltoid insufficiency can occur in patients with longstanding flatfoot deformity. Arthrodesis of the hindfoot increases the lever arm of the talus, thus placing a greater strain on the deltoid ligament. In this case, with early recognition of this problem, a second surgery resolved the deltoid insufficiency and hindfoot valgus, with good results for the patient.
Posted: 7/1/2019
Authors
Amelia Hummel, BA
Research Assistant
Foot and Ankle Service
Hospital for Special Surgery

Associate Attending Orthopedic Surgeon, Hospital for Special Surgery
Associate Professor of Orthopedic Surgery, Weill Cornell Medical College
Associate Attending Orthopedic Surgeon, NewYork-Presbyterian Hospital
References
- Chan JR, Williams BR, Pallavi N, et al. The contribution of medializing calcaneal osteotomy on hindfoot alignment in the reconstruction of the stage II adult acquired flatfoot deformity. Foot Ankle Int. 2013;34(2):159–166.
- Conti M S, Elli, SJ, Chan JR, Do HT, Deland JT. Optimal position of the heel following reconstruction of the stage II adult-acquired flatfoot deformity. Foot Ankle Int. 36(8):919–927.
- Dodd A, Daniels TR. Total ankle replacement in the presence of talar varus or valgus deformities. Foot Ankle Clin. 2017;22(3):277–300.