Limb Lengthening – An Overview
An interview with S. Robert Rozbruch, MD
As recently as the late 1980s, individuals in the United States who had limb length discrepancies – the result of a poorly healed fracture, disease, or a congenital defect – had few treatment options. Today, thanks to an innovative surgical technique originally developed more than half a century ago in Russia, these individuals may be candidates for treatment that can not only correct the discrepancy, but also address any associated deformity.
- What is limb lengthening surgery?
- Recovery and rehabilitation
- Eligibility for limb lengthening surgery
- Looking to the future
What is limb lengthening?
Limb lengthening is achieved using the body's own capacity to regenerate new bone as well as the soft tissues, ligaments, blood vessels, and nerves that surround and support it. The process begins with an operation called an osteotomy, in which the orthopedic surgeon cuts the bone to be lengthened. The limb (usually the upper or lower leg) is then stabilized using one of several different external and/or internal fixation devices or frames.
Two phases of recovery follow. In the first, or distraction phase, the bone that has been cut is very gradually pulled apart, in a process that promotes distraction osteogenesis or new bone growth at the site of the osteotomy. Continued growth of new bone tissue is accomplished by distracting or spreading the gap typically four times a day, one quarter millimeter (¼ mm) with each adjustment, for a total of one millimeter (1 mm) a day. As the space between the ends of the bone opens up, the body continues to produce new tissue in the gap until the desired length of bone has been generated. Additional strategies are available to correct any deformity that may be present, such as a misalignment of the bone resulting from trauma or a birth defect. Early on in this phase, patients walk with the aid of crutches in order to remain mobile.
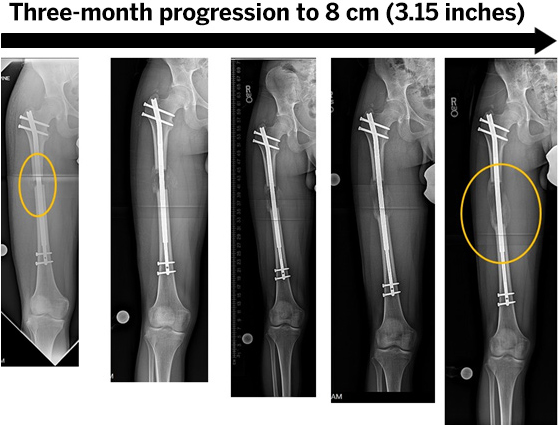
The above X-ray images are of an osteotomy of the femur that was performed through a percutaneous approach. Gradual lengthening (8 cm) was accomplished with an internal lengthening nail to optimize leg lengths. Note the early new bone formation in the gap.
During the second phase of treatment the bone consolidates and heals. The patient gradually puts more weight on the affected limb, and starts walking without any assistance.

The gradual process of lengthening can be accomplished with either an external fixator or an internal lengthening nail.
External fixation is a frame built on the outside of the limb connected to the bone via pins (rods), screws and wires. Adjustments to the external fixator can be used to gradually lengthen and straighten the short and malaligned limb.
The internal lengthening nail (ILN) is a telescopic, motorized intramedullary nail or rod that is inserted into the marrow cavity of the bone. With a remote control device, the magnet in the nail is rotated and this gradually elongates the telescopic nail and the bone. With this method, the bone is straightened at the time of surgery when the ILN is inserted, and the lengthening is then done gradually over the next several weeks.
According to S. Robert Rozbruch, MD, Chief of the Limb Lengthening and Complex Reconstruction Service (LLCRS) at the Hospital for Special Surgery (HSS) and Professor of Clinical Orthopaedic Surgery at Weill Cornell Medicine, once the lengthened bone is healed, this new bone is as strong as any other bone in the body and does not weaken or deteriorate over time
Osteotomy and placement of most fixation devices may be done using epidural anesthesia – the same type of anesthesia that many women receive during childbirth – so that they may be awake during their surgery if they so choose. The average hospital stay is two days. The procedure involves no large incisions or bone grafts.
Generally, patients who did not have a problem with pre-existing pain do not report significant pain in association with the surgery or the recovery. At HSS, our pain panagement team works closely with all patients to keep them comfortable throughout the process.
Most patients treated at HSS for this problem have leg length inequality that is the result of a congenital defect, a growth plate injury in childhood, or malunion of a fracture in which the bones heal in a deformed position or a non-union in which the bones do not heal at all. However, limb lengthening may also be used to correct a deformity of the arm. And the procedure has been used to lengthen both the arms and legs of individuals with exceptionally short stature as in dwarfism or precocious puberty.
An additional group of patients who can benefit from the techniques used in limb lengthening are those with a limb at risk for amputation owing to missing bone tissue, lost from an infection, trauma or tumor. In what is called a bifocal procedure for limb salvage, an incision is made at the opposite end of the bone from the affected site. As this area is gradually pulled apart, the ends of the bone that abut the gap are pushed together. As with other limb lengthening procedures the area at the site of the osteotomy generates new bone; the area where there has been an absence of bone comes together and heals as any other fracture would. Even in situations like this, we are often able to avoid an external fixator and use the Bone Transport Nail, a new technology developed by at HSS by Dr. Rozbruch and Austin T. Fragomen, MD.
Overall, limb lengthening surgeries have a high success rate (about 95%). Scarring is usually minimal since only small incisions are required in most procedures. Although minor problems may occur with pins and stiffening in the joints, serious complications from limb lengthening surgery are rare. Those that do occur are usually in seen in patients who are already considered to be high risk, such as those who are being treated for limb salvage.
What is the recovery time for the limb lengthening procedure?
Recovery time from the limb lengthening procedure varies among patients, with the consolidation phase sometimes lasting a considerable period – especially in adults. As a general rule, children heal in half the time as it takes for adult patients. For example, when the desired goal is 1½ inches of new bone growth, a child will wear the fixation device for three months. In adults, although bone healing takes longer, the use of the internal lengthening nail makes the process more simple as there is no external fixator needing to be worn.
Throughout recovery, physical therapy plays a crucial role in keeping the patient's joints flexible and in maintaining muscle strength. Patients are advised to eat a nutritious diet and to take calcium supplements. To hasten bone healing, gradual weight-bearing is encouraged and the patient takes supplements like vitamin D3 and calcium to hasten bone healing.
Who is eligible for limb lengthening surgery?
Treatment for limb length discrepancy should begin with a thorough evaluation from an orthopedic surgeon experienced in the procedure. Patients may be surprised to learn that what they thought was a discrepancy in leg length, for example, is actually an entirely different medical problem, such as scoliosis (an abnormal curve of the spine) or a hip deformity. Or, they may have a mistaken perception about the length of their limb length inequality. At the Hospital for Special Surgery, orthopedic surgeons on the Limb Lengthening Service obtain a special series of X-rays to precisely assess and confirm each diagnosis.
When true discrepancy does exist, even when it is not the result of trauma, this asymmetry may lead to back, knee and ankle pain. In the case of malunion (a fracture that has not healed properly), osteoarthritis may develop. In some cases, a patient has lived with a limb length discrepancy for many years without experiencing problems and then develops troublesome symptoms in middle age.
"In addition to meeting physical criteria for limb lengthening, it's important that the patient be highly motivated." says Dr. Rozbruch. Patients take an active role in their care, actually lengthening their bone with remote control adjustments, participating in physical therapy, and meeting with their physician in person or virtually every two to three weeks throughout the recovery process.
Limb lengthening surgery can be done safely and effectively in both children and adults–including those in their 20s, 30s, 40s, 50s, and even 60s. In pediatric patients, the orthopedic surgeon takes special care to avoid injuring the growth plate, and both normal growth and distraction osteogenesis continues during recovery.
In some cases, as with children who have congenital short femur, it may be advisable to address the problem in two stages. In this condition, the child has a percentage discrepancy that increases as they grow; for example, a two-inch discrepancy when the patient is first examined can be anticipated to increase to a three-inch discrepancy within five or six years. For the patient pictured below, Dr. Rozbruch corrected a two-inch discrepancy in an initial procedure; another procedure will probably be necessary as the remaining discrepancy becomes evident.

The above image is of a gradual two-inch lengthening of the femur, which was done with a frame over a two-month period. The below images were taken seven months later.


Because this type of deformity can be as great as six inches, it is generally preferable to break it up into two or even more surgeries.
Looking to the future
Despite the historical roots of limb lengthening surgery, the field is "in its infancy," according to Dr. Rozbruch. "There has been a dramatic shift in perception of this surgery in the United States and interest in the field is expanding rapidly, with many promising developments ahead of us, including new devices that promote faster healing."
Among recent advances is the FDA approval of a fully implantable internal device for bone transport which can be used to reconstruct bone defects without the need for external fixation.
In addition, phenomena that occur during limb lengthening procedures, such as nerve regeneration and development of new vasculature, may have significant implications in the future for a range of orthopedic and other medical conditions.
(Find a limb lengthening surgeon at HSS.)
Updated: 4/28/2020
Summary Prepared by Nancy Novick *Diagnostic imaging examinations provided by HSS Radiologists
Authors

Chief, Limb Lengthening and Complex Reconstruction Service, Hospital for Special Surgery
Director, Osseointegration Limb Replacement Center, Hospital for Special Surgery