Cartilage Injuries
Case Example
Femoral Head Fracture with Osteochondral Lesion
A previously healthy 18-year-old male was involved in a motor vehicle accident as a belted driver whose automobile struck a pole and was taken to a local hospital where evaluation revealed an isolated Pipkin IV Type posterosuperior fracture-dislocation of the right hip. Closed reduction was performed within two hours of the accident. A post-reduction CT revealed a congruent, located hip joint and reduced femoral head fracture. A small, peripheral posterior wall fracture of the acetabulum was identified. The patient was transferred to another hospital where he was admitted for observation. Four days later, he was discharged home, non-weight bearing with crutches. He presented to the HSS Orthopedic Trauma Service 20 days following the injury for definitive management by Dr. David L. Helfet with recurrent fracture dislocation of the hip and increased pain with passive and active motion. Vascular and neurologic examination was normal except for grade 3/5 motor strength in the foot plantar flexors. CT and MRI studies were performed to for further assessment. Comminuted fragments of bone were seen within and behind the joint, involving the posterior wall of the acetabulum and femoral head. A large medial fragment of the femoral head was found to be completely displaced from the remaining, lateral head. The middle third of the femoral head appeared to have a significant impaction injury.
A Kocher-Langenbeck approach with a trochanteric flip and anterior dislocation of the hip was performed and the multiple fracture fragments were visualized. One was a free, thin osteochondral fragment found along the anterior surface of the femoral head. Considering the fact that the middle one-third of the femoral head was missing but involved the weight-bearing area, it was elected to obtain a frozen, femoral head osteochondral allograft. Once thawed, it was cut into place with an oscillating saw so as to fit into the defect. Autograft morselized bone was obtained from the greater trochanter and was placed underneath the allograft, the reconstructed medial femoral head fragment, and the osteochondral fragment. Two screws were placed into each loose fragment and aimed towards the intact femoral head. The screw heads were seated below the articular surface of the femoral head fragments. The femoral head was found to be congruous. The small, loose fragments from the periphery of the posterior wall were debrided as they were not felt to be requisite to the stability of the hip joint. The hip was located and congruity confirmed. He returned for regular follow-up visits and at 32 months and was working full time and returned to pre-injury activities. Radiographs of the hip showed a healed fracture of the femoral head and trochanteric osteotomy. There was a small amount of heterotopic ossification (Brooker stage I). There was no evidence of avascular necrosis (AVN). Crossing trabeculae were seen between the allograft and lateral femoral head with no evidence of collapse or ischemia in either.

Anteroposterior x-ray of right hip on presentation to the hospital after motor vehicle accident and (right image) CT scan showing coronal and axial images of femoral head and posterior wall of the acetabulum after hip re-dislocated (posterior wall fracture indicated with black arrow).
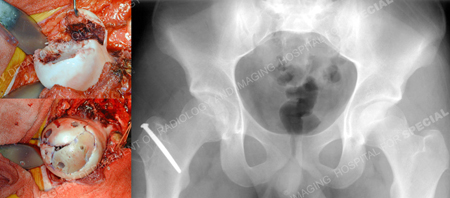
Intraoperative photos of femoral head at time of exposure (top left image) and after fixation with screws (bottom left image) and postoperative anteroposterior x-ray of pelvis (right image).
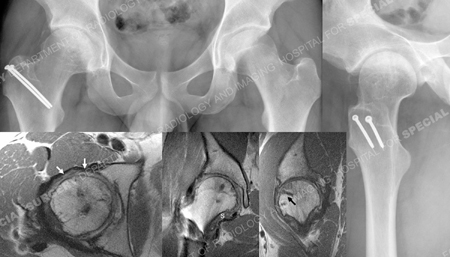
Anteroposterior and lateral X-rays of hip 21 months after surgery and MRI images of hip 7 months after surgery; and MRI images (from left to right) axial MR image demonstrates restoration of femoral head contour after reduction and graft fixation and articular cartilage remains intact (white arrows), coronal MR image suggestive of graft having been incorporated, mild flattening of medial border with otherwise normal contour and synovitis evident; indicated with “s”, sagittal MR image; linear low signal (black arrow) is from Bionix screw.
Research Publication
The HSS Orthopedic Trauma Service has conducted many studies. Please see our publication on femoral head fractures and treatment of fracture dislocations.