Carpal Tunnel Syndrome: Myths, Facts, Diagnosis, and Treatment
An interview with Aaron Daluiski, MD
- Introduction
- What is carpal tunnel syndrome?
- What causes it?
- How is it diagnosed?
- What are the treatment options?
- What are the chances of pain alleviation and recovery after surgery?
- Conclusion
Introduction
The use of computer keyboards, cell phones, PDA’s, gaming controls, and other handheld devices in our present “Information Age” has been widely claimed in the media to lead to a variety of repetitive stress injuries, including De Quervain’s Syndrome, so-called “Techno Thumb,” and, particularly, carpal tunnel syndrome.
Despite these claims, however, studies performed on this cause-and-effect relationship in recent years have produced no conclusive evidence attributing carpal tunnel syndrome to overuse or incorrect usage of these devices. Carpal tunnel syndrome develops over many years by a gradual reduction in the space within the carpal tunnel for the median nerve. Although there has not been a direct causative link between repetitive use and carpal tunnel syndrome, wrist position (flexion or extension) can increase pressure on the median nerve and either cause symptoms or make them worse.
In order to dispel the myths and rumors attached to the causes, diagnoses, and potential treatment options of the condition, it’s important to understand exactly what it is. We recently sat down with Aaron Daluiski, MD, Assistant Attending Orthopedic Surgeon at Hospital for Special Surgery, to gather his views and clarify the recent misunderstandings about carpal tunnel syndrome.
What is carpal tunnel syndrome?
Carpal tunnel syndrome (CTS) is a compression neuropathy (disease of the nervous system) caused by an increase in pressure on the median nerve. The carpal tunnel is a space in the wrist bound on three sides by bone and covered with a ligament through which nine tendons and one nerve (the median nerve) travel to the fingers. This nerve supplies sensation to the thumb, index, middle, and half of the ring finger (excluding the pinky), while providing innervation of muscles that control thumb motion.
When the median nerve is compressed, it results in increased sensitivity, tingling, pain, weakness, or numbness in the fingers, hand, and wrist; the pinky finger remains largely unaffected. Night symptoms of numbness and/or pain are common in those suffering from this condition. In addition, it is not uncommon for many to experience symptoms bilaterally (on both sides of the body).
What causes it?
The predisposing factors that cause median nerve compression and carpal tunnel syndrome are unknown. Most experts believe that the condition is made worse by prolonged wrist positioning (either flexion or extension), trauma (such as fractures of the wrist or hematoma formation in the carpal tunnel), osteoarthritis, forms of inflammatory arthritis such as rheumatoid arthritis, or inflammation of tendons (tendonitis) in the wrist. There is a higher incidence of carpal tunnel syndrome in patients with diabetes or thyroid disease as well as patients who are pregnant or on hemodialysis.
Activities such as bicycling, gymnastics, or playing tennis require the participant to place pressure directly over the region of the wrist, which may lead to compression of the median nerve and the symptoms of carpal tunnel syndrome.
Despite popular belief, heavy usage of computer keyboards has never been proven to be a direct cause of CTS. In addition, not all wrist pain is CTS. Using an incorrectly-positioned computer keyboard or mouse is linked to certain kinds of wrist pain; Laptop keyboards, especially, are frequently either too small or incorrectly elevated, resulting in wrist strain. However, the pain associated with the use of computers, while exhibiting similarities to CTS-associated pain, is not necessarily CTS itself. These similar types of pain can usually be corrected – primarily with ergonomically-minded corrections to the workspace and, if necessary, with a wrist splint.
“People naturally associate carpal tunnel syndrome with computer usage, and the media have perpetuated so much fear about it that it’s easy to understand why people make that connection,” notes Dr. Daluiski.
How is it diagnosed?
The diagnosis of carpal tunnel syndrome is made primarily by clinical examination and the patient’s history of symptoms. It is important to remember that not all wrist and finger pain is CTS. In addition, not all finger numbness or tingling is CTS. Confirmation of the diagnosis with the use of nerve electrodiagnostic testing is often useful.
Electrodiagnostic testing, made up of nerve conduction and electromyography (EMG) testing, is used to confirm the diagnosis of carpal tunnel syndrome and other nerve disorders. Nerve conduction studies (NCS) evaluate the conduction of electrical signals through the median nerve in the carpal tunnel and into the associated muscles. A conduction block, or slowing of the electrical signal through the nerve as it courses through the carpal tunnel, can be compared to the reduced flow of water through a garden hose that has a kink in it. This reduced flow of electricity results in the altered sensation and muscle weakness associated with this syndrome.
EMG testing studies the muscle itself. By examining how the muscle depolarizes when activated, it can be determined if the nerve input to that specific muscle is working properly. Very subtle loss of muscle function can be determined long before the patient experiences any subjective loss in strength, making this portion of the test very important for detecting early nerve damage.
“Electrodiagnostic testing, especially EMG studies, is important,” Dr. Daluiski explains. “EMG testing is the best measurement for determining if pressure on the median nerve has caused early denervation of the muscles at the base of the thumb. If I see evidence of denervation on the EMG portion of the test, I will usually recommend more aggressive treatment because it is more likely to mean the patient already has a significant degree of irreversible damage to the median nerve.”
What are the treatment options?
Treatment options for those with carpal tunnel syndrome depend upon the severity of each case. Regardless, the main objective is to relieve the pressure within the carpal tunnel. “It all comes down to making more room for the nerve,” explains Dr. Daluiski.
Options range from unproven and controversial theories to tested therapies such as braces, medication, and surgical correction.
Low tech solutions:
- avoiding pressure on the median nerve by being aware of risks and changing habits leading to increased pressure and pain
- splinting or bracing the wrist to avoid prolonged extension or flexion; splints are typically worn at nighttime while sleeping
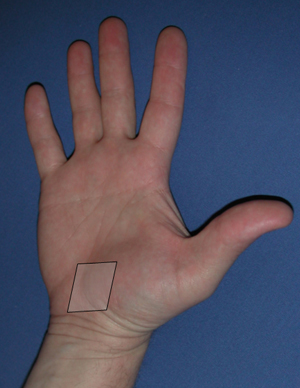
The shaded area in the above photo represents the carpal tunnel area where the median nerve is located.
Medications:
- anti-inflammatory medications, e.g., non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen
- steroid injections
While all of these options may offer some benefit, nighttime splinting and steroid injections are most frequently used in the nonoperative management of carpal tunnel syndrome. According to Dr. Daluiski, steroid injections into the carpal tunnel can be successful as an early treatment for patients who have experienced their symptoms for less than a year. Even in this particular patient population, however, only 40% will experience pain relief for a year following injection. Despite this statistic, however, Dr. Daluiski believes that many patients can benefit from this treatment. “It’s a great temporary solution for those who exhibit no serious denervation and muscle weakness and who require temporary relief,” he explains.
There are some important points to consider when undergoing steroid injection, stresses Dr. Daluiski. “The downside to this kind of treatment is that the patient could have continued progression of nerve damage even though their symptoms have improved.” He monitors his patients closely and never administers more than two injections. “Three is the magic number, but I usually use less. If a patient has had significant relief from a single injection and has a recurrence of severe pain after several years and still has no evidence of atrophy, I might recommend another injection, but only rarely.”
He suggests having a regular evaluation (which may include repeat electrodiagnostic studies) 6-12 months after the initial injection to watch for progression of nerve damage.
Surgery:
- Endoscopic surgery:
This is a minimally invasive technique in which the surgeon makes one or two small incisions in the wrist and palm, inserts an endoscopic imaging device at the end of a long tube to observe the area, and cuts the transverse carpal ligament. The procedure is usually performed under local or regional anesthesia with sedation.
The advantages of this kind of procedure include a reduced recovery period and a reduction of incisional pain due to the lack of incision in the palm. Disadvantages may include the expense of this procedure when compared to the traditional open method and a potentially higher rate of nerve injury or incomplete release.
Dr. Daluiski prefers the open method (described below) to the endoscopic method due to the aforementioned risks. “I don’t discourage patients from seeking the endoscopic method,” he explains, “but I don’t think the benefit is there when the potential risks are considered.”
- Open surgery:
This technique, like the endoscopic method, involves releasing the transverse carpal ligament (the roof of the carpal tunnel) to allow more room for the median nerve. It is a same-day procedure requiring local anesthesia with possible sedation and an approximate 1-inch incision, usually taking 8-10 minutes to complete. While the recovery time for open surgery can be longer than the endoscopic method (4-6 weeks until full restrictions are lifted for patients undergoing an open release), Dr. Daluiski provides reasoning why he is in favor of the open surgery technique for carpal tunnel syndrome:
“The realistic risks of this type of surgery are very small and the benefit to the patient to preserve nerve function and improve symptoms is usually far greater than this risk. It usually alleviates the pain, especially the night time numbness and tingling that patients experience. Although trained to do endoscopic releases, I get consistent results with the open technique and have not found the benefit of the endoscopic technique to be dramatically superior.”
Dr. Daluiski stresses that these procedures shouldn’t be done in anticipation of denervation or in the absence of symptoms. The procedure should, however, be considered in patients with severe symptoms and active denervation, and it should be done in a reasonable time frame (i.e., not to wait three years) because it might prove to be too late to prevent deterioration of muscle strength at that point.
What are the chances of pain alleviation and recovery after surgery?
While the surgical release of the transverse carpal ligament has risks, most patients have significant relief of pain, numbness, and tingling. If treatment is administered early enough to preserve nerve function, the most obvious improvement in the patient is pain relief -- particularly nighttime pain. “There is often dramatic improvement even the first night after surgery,” notes Dr. Daluiski.
If a carpal tunnel release is performed after significant denervation has led to atrophy of the thumb muscles, the surgery will not improve the loss of muscle strength. Once the muscle is denervated, it is impossible for the nerve to form a new connection to the muscle. While sensation in the hand can sometimes improve following surgery, muscle strength and motor function do not. However, recurrence of CTS symptoms after surgery is rare.
Conclusion
Carpal tunnel syndrome has attracted a sizeable amount of press in recent years, leading many of those with hand and wrist pain to believe that their symptoms are the result of this condition. The use of computers and similar devices has been attributed by the media to be a significant cause of CTS; there is, however, no clinical proof that this is true. Regardless of the cause of their symptoms, those with hand and wrist pain should consult their doctor to determine the nature and severity of their condition.
Unproven treatment theories for CTS abound. Those with the condition should exercise caution by accepting only proven treatments administered by licensed physicians. The proven options for carpal tunnel syndrome treatment range from splints and braces to medications and surgery, and it’s important to know how far your condition has progressed in order to choose the appropriate treatment, thereby preserving your mobility while easing your pain.
Summary by Mike Elvin
Authors

Attending Orthopedic Surgeon, Hospital for Special Surgery
Associate Professor of Clinical Orthopaedic Surgery, Weill Cornell Medical College