Antiphospholipid Syndrome and Skin Problems – Top 10 Series
Top 10 Points Patients Should Know About Skin Findings in Antiphospholipid Syndrome

- What is antiphospholipid syndrome (APS)?
- What are the most common skin problems associated with APS?
- What are the other causes of livedo reticularis or livedo racemosa?
- What are other less common skin problems associated with APS?
- How common are skin problems in people with APS?
- Does livedo reticularis and/or livedo racemosa increase your risk of future blood clots?
- What are the treatments for livedo reticularis and livedo racemosa?
- What are the treatments for livedoid vasculopathy and skin ulcers?
- What is the treatment for superficial thrombophlebitis?
- If I have livedo reticularis or racemosa, should I be tested for antiphospholipid antibodies?
1. What is antiphospholipid syndrome (APS)?
Antiphospholipid syndrome (APS) is a systemic autoimmune disorder in which the patient’s immune system makes antibodies that target their own body cells. These antibodies, known as antiphospholipid antibodies (aPL), increase the risk of blood clots and pregnancy-related clinical problems. Antiphospholipid antibodies can occur in healthy individuals, or in patients with other autoimmune disorders such as systemic lupus erythematosus (lupus) or rheumatoid arthritis. (Learn more about APS terminology and APS classification versus diagnosis.)
Patients with APS are at a greater risk of developing (a) venous thrombosis (a clot in the vein), which commonly develops in the leg and (b) arterial thrombosis (a clot in an artery), which commonly leads to a stroke or heart attack. However, APS can affect any organ system, including the skin.
2. What are the most common skin problems associated with APS?
Livedo is the most common skin problem associated with APS. However, there are two types of livedo: livedo reticularis and livedo racemosa.
Livedo reticularis
Livedo reticularis (Picture 1) is a netlike or mottled pattern of purplish discoloration on the skin, which reflects the network of blood vessels within the skin. The discoloration is not fixed, and the skin findings come and go in intensity. Disturbance of blood flow thought to be due to constriction of blood vessels (vasospasm) leads to reduced oxygen delivery to the skin. This leads to red blood cells, without oxygen, accumulating under the skin and resulting in discoloration.

Picture 1: Livedo reticularis on the arm.
Livedo reticularis is common among people who do not have APS or other diseases (often due to cold temperatures leading to temporary vasospasm of blood vessels). For this reason, it does not in itself suggest a person has APS.
Livedo racemosa
Livedo racemosa (Picture 2) is a persistent, fixed, purplish discoloration in a broken, branched, irregular fashion. It is usually found on the extremities. Unlike livedo reticularis, livedo racemosa does not go away easily with warming of the skin. In patients with livedo racemosa caused by APS, the binding of aPL to the surface of skin cells and blood vessels leads to the production of substances that increase the risk of blood clot formation. This also leads to occlusion, impaired blood flow and oxygen delivery to the skin.
Livedo racemosa is uncommon in the general population, and it is always caused by some kind of underlying condition. Thus, it can be an indication that a person may have APS.
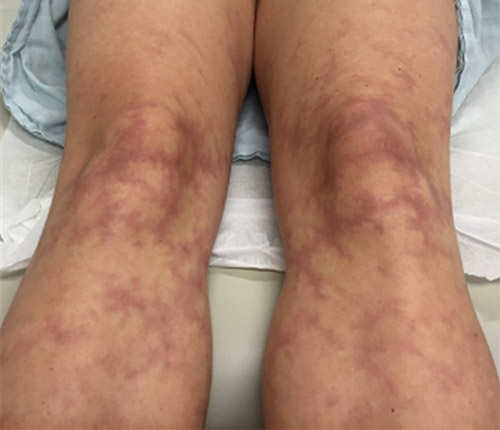
Picture 2: Livedo racemosa on lower extremities.
Picture courtesy of Dr. Joanna Harp
Unfortunately, data on livedo-related changes in the skin are limited and confusing, because the distinction between livedo reticularis and livedo racemosa has not been consistently well-described in medical literature.
3. What are the other causes of livedo reticularis or livedo racemosa?
Livedo reticularis
Livedo reticularis can be categorized as either primary (not associated with any disease) or secondary (due to an underlying disease).
Primary livedo reticularis
Primary livedo reticularis is relatively common in the general population – particularly in younger females. Different studies suggest that up to 50% of healthy young women develop livedo reticularis in cold environments. Livedo reticularis is so common among children, especially newborns, that it has its own specific term: cutis marmorata. Rewarming the child’s or infant’s skin should reverse the condition.
Secondary livedo reticularis
Secondary livedo reticularis is found among people with a variety of conditions, including:
- autoimmune diseases
- clotting and other occlusive disorders (including APS, as noted above)
- vasculitides (conditions caused by inflammation of blood vessels)
- certain infections
Rarely, secondary livedo reticularis can be caused by medications or malignancies.
It is important to understand that:
- Secondly livedo livedo reticularis is not specific to any of these conditions.
- It is generally very difficult to distinguish primary versus secondary livedo reticularis just based on the skin findings alone. For this reason, a physician’s medical evaluation and work-up for patients who have secondary livedo reticularis will be largely guided by additional symptoms, other skin or physical examination findings, and the patient’s medical and family history.
Livedo racemosa
Livedo racemosa is always due to an underlying condition, and in general is caused by the same categories of conditions that cause secondary livedo reticularis, as noted above.
4. What are other less common skin problems associated with APS?
Other, less common skin conditions associated with APS include:
- skin ulcerations
- superficial thrombophlebitis
- gangrene
Skin ulcerations
Livedoid vasculopathy results in painful skin ulcers and scarring due to chronic clotting in the blood vessels of the skin, generally in the lower part of the legs and top of the feet (Picture 3). Active ulcers have a bright red border and are very painful. Older areas of involvement tend to heal with white, slightly depressed scars. APS is one cause of livedoid vasculopathy but there are others.

Picture 3: Patient with livedo vasculopathy, presenting with ulcerations of lower legs.
Picture courtesy of Dr. Joanna Harp
Superficial thrombophlebitis
These are blood clots of the superficial veins of the skin. The area can be red, warm and swollen, with a lump underneath the skin.
Gangrene
A complete blockage of blood flow to the skin causes skin death due to lack of oxygen. This is called gangrene. The result is dusky, black, necrotic areas of skin, most often seen on fingers and toes.
Although anetoderma (wrinkly skin overlying round depressions in the skin) have been reported in aPL-positive patients, there is no well- proven association between anetoderma and APS.
5. How common are skin problems in people with APS?
In general, half of APS patients experience associated skin problems, ranging from livedo reticularis to skin ulcers. More specifically, approximately 25% of patients with APS have livedo reticularis and/or livedo racemosa. In addition, among aPL-positive patients:
- 8% have skin ulcerations
- 2% have skin necrosis
- 9% have superficial thrombophlebitis
6. Does livedo reticularis and/or livedo racemosa increase your risk of future blood clots?
There are clear correlations between livedo racemosa and vascular diseases, and this is not limited to APS patients. Studies suggest that patients with livedo racemosa are more likely to develop the following:
- cerebrovascular events (such as stroke)
- arterial clots
- high blood pressure
- heart value abnormalities
7. What are the treatments for livedo reticularis and livedo racemosa?
Generally, no treatment is needed for livedo reticularis. Treatment for livedo racemosa largely depends on the underlying cause or association, if found. Treating the underlying cause may help improve the appearance of livedo racemosa.
8. What are the treatments for livedoid vasculopathy and skin ulcers?
Treatment for livedoid vasculopathy and skin ulcers include:
- Localized wound care and preventing infection.
- Pain management.
- Treatment for venous stasis (the decreased flow and pooling of blood in the veins) – if this condition is also present – because this improves wound healing.
- Antiplatelet agents (such as aspirin, clopidogrel, prasugrel, ticagrelor, dipyridamole).
- Blood thinners (anticoagulation) – Currently, the treatment for venous and arterial blood clots in APS patients is long-term use of a blood thinner (warfarin). However, warfarin generally does not work well to treat aPL-related skin ulcers. Based on studies in patients who have livedoid vasculopathy due to causes other than APS, a new generation of blood thinners – dabigatran etexilate (Pradaxa) and rivaroxaban – have shown to be more effective. These medications, however, are not recommended for patients with APS if they have history of blood clots.
- Immunosupressive medications – a pilot study demonstrated that rituximab, an anti-B-cell agent, can be effective in the management of APS patients with skin ulcers.
- Hyperbaris oxygen therapy: This is a well-established treatment for chronic wounds and is thought to work by increasing oxygen delivery to the tissue.
9. What is the treatment for superficial thrombophlebitis?
Current treatment for any patient involves applying heat to the painful area, elevation, using an over-the-counter nonsteroidal anti-inflammatory drug (NSAID), and possibly wearing compression sleeves, stockings or socks.
For aPL-positive patients, it is not clear whether the treatment of superficial thrombophlebitis should be different than that for the general population. That is, do they need blood thinners? Despite the lack of strong evidence, many physicians prefer to use blood thinners in aPL-positive patients with superficial thrombophlebitis only.
10. If I have livedo reticularis or racemosa, should I be tested for antiphospholipid antibodies?
If you have additional symptoms or laboratory findings such as those listed below, then you should be tested for aPL:
- Unexplained blood clots, especially at a young age.
- Low platelet counts.
- Miscarriages.
- Another systemic autoimmune disease such as lupus.
- Abnormal results in an activated partial thromboplastin time (aPTT) screening test. This test helps evaluate a person's ability to appropriately form blood clots.
- Skin findings are that are fixed and do not improve with rewarming.
- Development of bruise-like areas or ulcers associated with the livedo findings.
Posted: 1/19/2021
Authors
Victoria Danan, BA
Charles E. Schmidt College of Medicine
Florida Atlantic University
Joann Harp, MD
Associate Professor of Medicine, Weill Cornell Medicine
Attending Rheumatologist, Hospital for Special Surgery
Professor of Medicine, Weill Cornell Medical College
Related articles
Antiphospholipid Syndrome (APS) Patient Stories
References
- Alegre VA, Gastineau DA, Winkelmann RK. Skin lesions associated with circulating lupus anticoagulant. British Journal of Dermatology. 1989;120:419-29.
- Asherson RA, Francès C, Iaccarino L, et al. The antiphospholipid antibody syndrome: diagnosis, skin manifestations and current therapy. Clinical and Experimental Rheumatology. 2006;24:S46-S51.
- Blume JJ, Miller CC. Antiphospholipid Syndrome: A Review and Update for the Dermatologist. MDedge Dermatology. 2006;78:409-415.
- Cervera R, Asherson RA, Acevedo ML, et al. Antiphospholipid syndrome associated with infections: clinical and microbiological characteristics of 100 patients. Annals of the Rheumatic Disease. 2004;63:1312-1317.
- Cervera R, Piette JC, Font J, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum. 2002;46:1019-1027.
- Cervera R, Tektonidou MG, Espinosa G, et al. Task Force on Catastrophic Antiphospholipid Syndrome (APS) and Non-criteria APS Manifestations (I): catastrophic APS, APS nephropathy and heart valve lesions. Lupus. 2011;20:165-173.
- Cervera R, Tektonidou MG, Espinosa G, et al. Task Force on Catastrophic Antiphospholipid Syndrome (APS) and Non-criteria APS Manifestations (II): thrombocytopenia and skin manifestations. Lupus. 2011;20:174-181.
- Costa R, Fazal S, Kaplan RB, Spero J, Costa R. Successful plasma exchange combined with rituximab therapy in aggressive APS- related cutaneous necrosis. Clinical Rheumatology. 2013;32 Suppl1:S79-82.
- Defelice T, Lu P, Loyd A, Patel R, Franks AG Jr. Livedo racemosa, secondary to drug-induced systemic lupus erythematosus. Dermatol Online Journal. 2010;16:24.
- DiFrancesco LM, Burkart P, Hoehn JG. A cutaneous manifestation of antiphospholipid antibody syndrome. Annals of Plastic Surgery. 2003;51:517-522.
- Diógenes MJ, Diógenes PC, de Morais Carneiro RM, Neto CC, Duarte FB, Holanda RR. Cutaneous manifestations associated with antiphospholipid antibodies. Int J Dermatol. 2004;43:632-637.
- El‐Rayes BF, Edelstein M. Unusual case of antiphospholipid antibody syndrome presenting with extensive cutaneous infarcts in a patient on long‐term procainamide therapy. Am J Hematol. 2003;72:154.
- Erkan D, Vega J, Ramón G, Kozora E, Lockshin MD. A pilot open-label phase II trial of rituximab for non-criteria manifestations of antiphospholipid syndrome. Arthritis Rheum. 2013;65:464-471.
- Francès C, Niang S, Laffitte E, Pelletier Fl, Costedoat N, Piette JC. Dermatologic manifestations of the antiphospholipid syndrome: two hundred consecutive cases. Arthritis Rheum. 2005;52:1785-1793.
- Gibbs MB, English JC 3rd, Zirwas MJ. Livedo reticularis: an update. Journal of American Academic Dermatology. 2005;52:1009-1019.
- Gillian E. Gibson, W.P. Daniel Su, Mark R. Pittelkow. Antiphospholipid syndrome and the skin. Journal of the American Academy of Dermatology. 1997;36: 970-982.
- Hairston BR, Davis MDP, Gibson LE, Drage LA. Treatment of Livedoid Vasculopathy With Low-Molecular-Weight Heparin: Report of 2 Cases. Arch Dermatol. 2003;139:987–990.
- Hellmann DB, Imboden Jr. JB. Livedo Reticularis & Livedo Racemosa. In: Papadakis MA, McPhee SJ, Rabow MW. eds. Current Medical Diagnosis and Treatment. 2020.
- Lima RS, Maquiné GÁ, Talhari C, Encarnação IC, Schettini AP, Santos M. Livedoid vasculopathy as a marker of systemic disease: report of two cases. An Bras Dermatol. 2014;89:822–824.
- Martínez-Valle F, Ordi-Ros J, Selva-O'Callaghan A, Balada E, Solans-Laque R, Vilardell-Tarres M. Livedo racemosa as a marker of increased risk of recurrent thrombosis in patients with negative anti-phospholipid antibodies. Med Clin (Barc). 2009;132:767-771.
- Ugolini-Lopes MR, Criado PR, Parsi K, et al. Treatment of non-criteria manifestations in APS. In: Antiphospholipid Syndrome: Current Research Highlights and Clinical Insights. Eds: Erkan D, Lockshin MD. Springer, 2017, p: 247
- Nahass GT. Antiphospholipid antibodies and the antiphospholipid antibody syndrome. J Am Acad Dermatol. 1997;36:149-172.
- Sajjan VV, Lunge S, Swamy MB, Pandit AM. Livedo reticularis: A review of the literature. Indian Dermatol Online J. 2015;6:315-321.
- Ünlü O, Zuily S, Erkan D. The clinical significance of antiphospholipid antibodies in systemic lupus erythematosus. Eur J Rheumatol. 2016;3:75-84.
- Uthman, I. W., & Khamashta, M. A. Livedo racemosa: a striking dermatological sign for the antiphospholipid syndrome. The Journal of rheumatology. 2006;33:2379-2382.